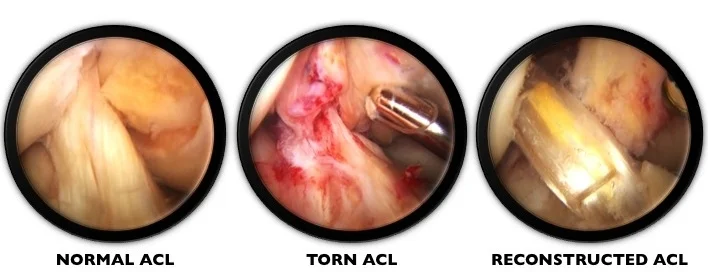
VIDEO: ACL Reconstruction
/An oldie, but a goodie from 2013!
husband + wife team providing surgical care to elite + recreational athletes in the seattle area
The musings + thoughts of the Wahl Team, a Seattle-based surgical orthopedic husband + wife team, who specialize in surgical sports medicine + athletic trauma.
An oldie, but a goodie from 2013!
An interview about ACL revision surgery with IRG PT on Komo News 97.7 FM.
When a patient tears their native ACL and then unfortunately tears their reconstructed ACL then it is prudent to consider an ALL reconstruction (anterolateral ligament or extra-articular augmentation) when revising the intra-articular ACL.
This structure helps control rotational instability. We often use this as an “insurance policy”…particularly if the patient tore their graft despite having the appropriate graft and good tunnel placement.
We also strongly consider an ALL when the patients “well” knee behaves ACL deficient with a pivot, despite having an intact ACL.
The technique is as follows…
1️⃣ Split ITB (iliotibial band).
2️⃣ Fix graft at Gerdy’s tubercle.
3️⃣ Route the graft beneath the LCL to the lateral epicondyle.
4️⃣ Find the isometric position.
5️⃣ Fix graft at isometric position.
6️⃣ Close ITB.
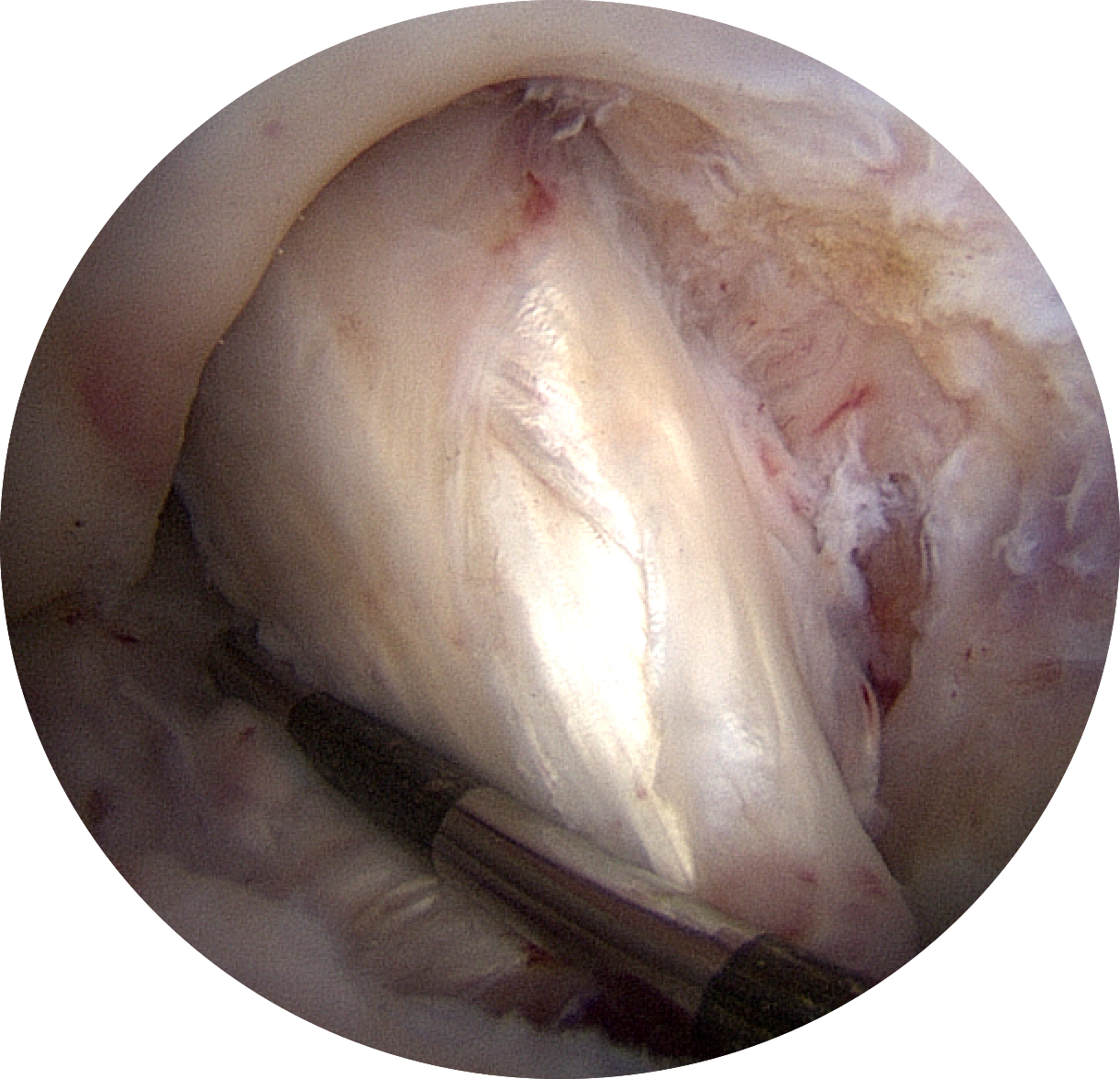
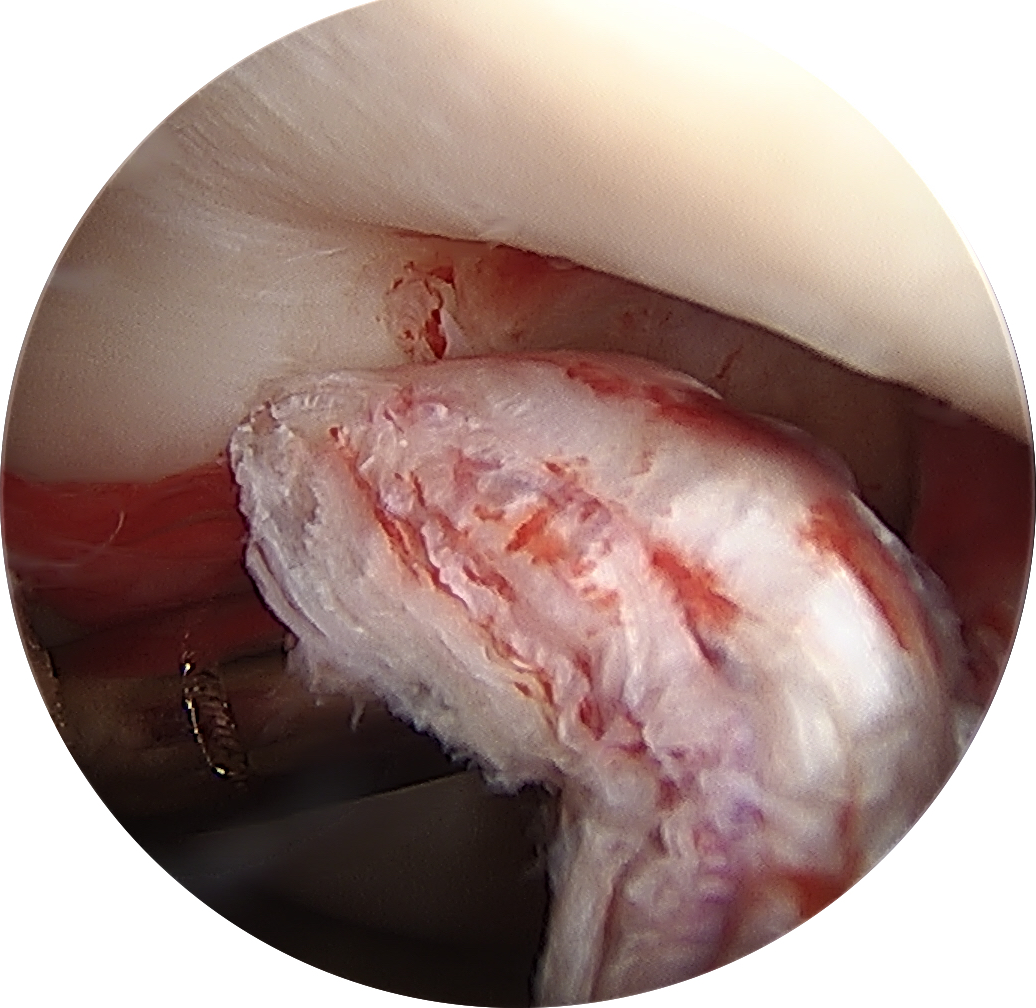
Patients with acute ACL tears can sometimes present with missing terminal extension (inability to fully straighten the knee). One must always suspect a bucket-handle meniscus tear in this situation, but sometimes it is due to “stump entrapment” where a portion of the torn ACL flips forward and gets pinched between the femur and tibia, acting as a mechanical obstruction that limits full extension of the knee.
1️⃣ + 2️⃣ Arthroscopy views of the ACL fragment caught in the intercondylar notch.
3️⃣ + 4️⃣ Sagittal and coronal MRI views of the ACL fragment flipped forward.

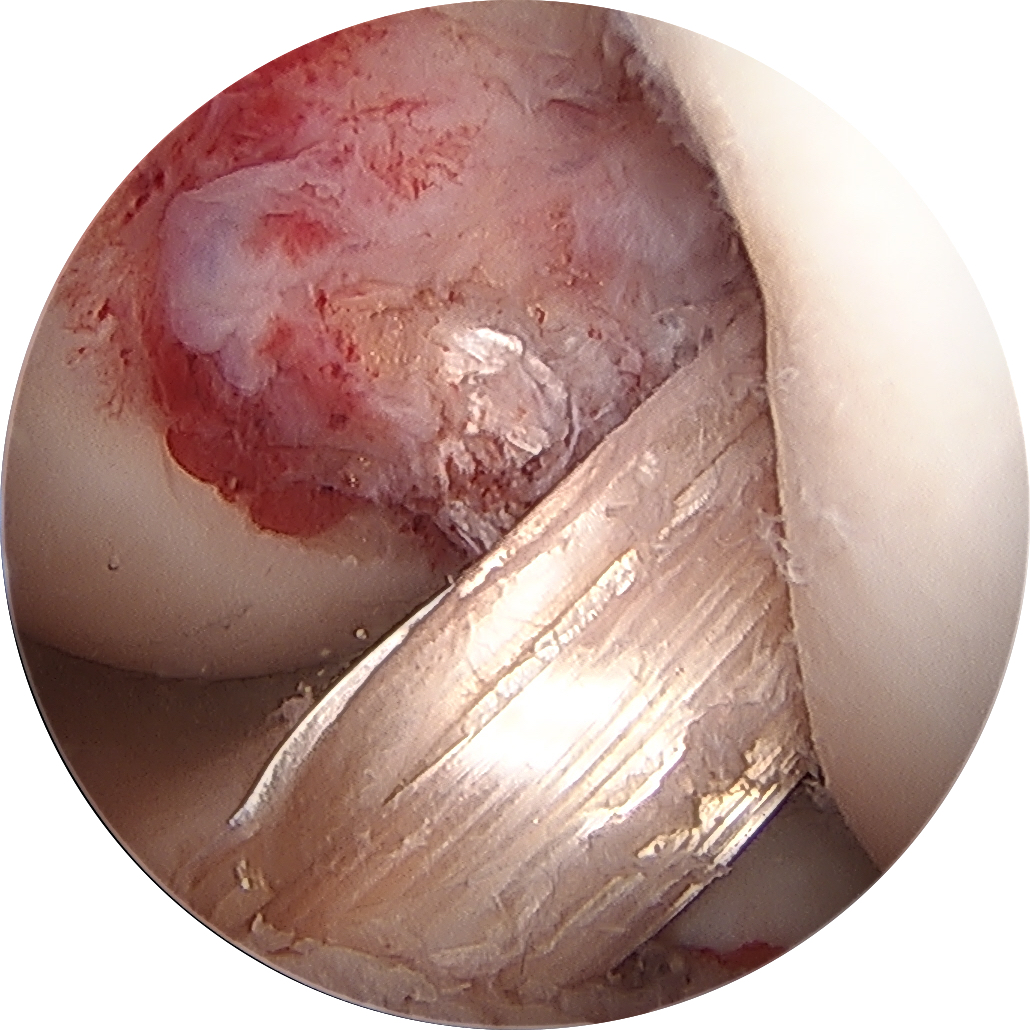
The graft looks good....but is it ready for the patient to return to soccer?
Graft healing is an extremely complex process influenced by many variables (type of graft used, method of graft fixation + tensioning, graft motion, etc). Shockingly, during the healing process, the ACL graft tissue gradually weakens with decreased structural properties and the graft is most vulnerable at 6-7 weeks after surgery and the graft never returns to its original strength at the time of implantation!
This is why, it's important to follow your surgeons PT protocol, they know when the graft can endure more stress. No matter how good you feel or how ready you think you might be, your surgeon has a specific timeline that allows for return to running, jumping, athletics, etc. The recovery timeline is based on the biology of the graft...not how it looks on MRI, how it feels on exam or how ready you feel! Be patient...it's in your knees best interest!
This ACL graft involves a bone plug from the tibial tubercle, the central 1/3 of the patellar tendon and a bone plug form the patella.
1️⃣ Patellar Tendon.
2️⃣ Bone plug from tibial tubercle.
3️⃣ We take a small piece of extra bone from the tibial tubercle plug and use it as bone graft in the recipient patellar bone plug site.
4️⃣ Middle 1/3 of the patellar tendon removed.
5️⃣ Closure of the patellar tendon with the knee at 90 degrees of flexion.
6️⃣ Closure of the peritenon with the knee at 90 degrees of flexion.
7️⃣ BTB autograft.
8️⃣ Final ACL reconstruction with BTB autograft.
When performing an ACL reconstruction with hamstring autograft (using the patients own hamstring tendons), 2 hamstring tendons are used to make up the graft; the semitendinosus and gracilis. The 2 strands of tendon are sewn together to make one bundle. Then the bundle is folded onto itself, essentially making a 4-strand graft.


There are no absolutes about who is ‘too young’ or ‘too old’ to consider reconstruction, the decision should really be made with respect to how knee instability affects a person’s ability to remain active and healthy.
Read MoreThere are some knee conditions that in my practice are “deal-breakers” for using particular ACL grafts.
Read MoreMultiple studies have demonstrated that females have a 4x to 10x higher risk of ACL-injury compared with same-sport males, and up to 4x higher rate of re-injury or further surgical treatment after they’ve undergone ACL reconstruction.[i]
Read MoreThe allograft is the “Honda scooter of grafts” – It is easy to drive, you can park it anywhere, it’s dirt cheap with respect to graft pain, but they don’t work well to haul things or race, and there might be some reliability and safety issues. You might not want it as your only vehicle.
Read MoreThe QT graft is a little like a “Hybrid Hatchback of grafts” – it actually does a lot pretty well, but not everything, not very ‘costly’ in terms of pain, but a lot of people just never think about buying one.
Read MoreHamstring autograft is the “4WD SUV of grafts” – It is reliable, it is flexible, it is a workhorse that works great for most people with few exceptions (from taking out the groceries all the way to tennis practice to the marathon). It isn’t too ‘costly’ with respect to pain or arthritis, but high performance individual, elite athletes and folks exposed routinely to contact sports might be looking for a little more.
Read MoreFor me, the BTB is the “Luxury Sports Car of Grafts” – it’s built for speed and power, it’s sexy, it wins races, but it comes at a potential cost, and it may be more than some people need. I prefer using the BTB graft for my patients who are in the athletic population, unless there are specific patient variables that make me think it is not the best choice or contraindicated.
Read MoreNot everyone who has an ACL tear needs to have ACL surgery; so, before signing up for surgery to reconstruct your ACL, think about your activity level, current level of function and comfort, activity goals, etc and decide with your surgeon what the best treatment option is for you and your knee.
Read MoreACL reconstruction...as good as it is, it is still not perfect. ACL reconstruction is one of the most successful procedures we have in orthopaedics, that is, depending on the type of patient...
Read MoreDr. Christopher J. Wahl, offering expertise in surgical sports medicine, trauma dan orthopedics in Seattle, WA; specializing in complex knee and shoulder injuries.
©2016-2025 . wahlmd . all rights reserved | disclaimer
website created by suzanne l. wahl